Diastasis rectus abdominis
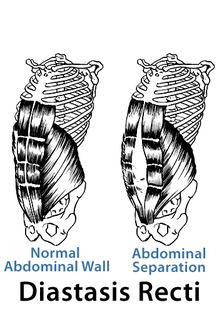
A diastasis rectus abdominis (DRA) is a condition common in pre- and postpartum women. It is the splitting of the two rectus abdominis muscles, which can range in size from 2-3 cm to 12-20 cm in width and in length from 12-15 cm to the entire length of the rectus abdominis muscles. The split can occur anywhere along the linea alba, which is the central insertion point of the rectus abdominis, internal obliques, external obliques, and transverse abdominis. However, the level of the umbilicus seems to be the most common, followed by below the umbilicus, and then above the umbilicus.
A DRA hinders the function of the abdominal wall and its contribution to posture, trunk stability, respiration, visceral support, pelvic floor facilitation, and delivery of the fetus. It is thought that a DRA contributes to chronic pelvic and low back pain, as well as bowel and bladder dysfunction.
A DRA hinders the function of the abdominal wall and its contribution to posture, trunk stability, respiration, visceral support, pelvic floor facilitation, and delivery of the fetus. It is thought that a DRA contributes to chronic pelvic and low back pain, as well as bowel and bladder dysfunction.
Predisposing factors
|
Prevalence
|
DRA measurement
- Patient lies supine in a hook lying position
- The therapist places his/her fingers horizontally at the linea alba.
- The patient is instructed to perform a curl up to the point of bringing the head and superior aspect of the scapula off of the treatment table.
- If a DRA is present, the therapist will palpate a separation between the rectus muscles. The patient holds the position while the therapist measures the distance. The criteria for a DRA are as follows: (1) >2.7 cm at the level of the umbilicus (2) >1.0 cm above the umbilicus or (3) >0.9 cm below the umbilicus
- The test is performed at the level of the umbilicus, as well as two inches above and below the umbilicus.

Physical therapy implications
Some studies have shown that 66% of women have a DRA in the third trimester, and 53% continue to have one immediately post-partum. After 5-7 weeks, 36% continue to have a DRA, and after 8 weeks, the diastasis no longer decreases without intervention. This highlights the prevalence of the disorder and the need for effective intervention to prevent the sequelae from this disorder. The goal of treatment should be due to minimize the distance between the recti muscles, promote total core stability in functional activities, resolve pelvic and/or low back pain, and prevent bowel and bladder dysfunction.
Recommendations
|
Exercises to avoid
|
References
- Dutton M. Orthopaedic Examination, Evaluation, and Intervention. 2 ed: McGraw-Hill, Medical Publishing Division; 2008.
- Lee D. Diastasis rectus abdominis and portpartum health. 2012; http://dianelee.ca/education/article_diastasis.php.
- Parker MA, Millar AL, Dugan SA. Diastasis rectus abdominis and lumbo-pelvic pain and dysfunction -- are they related? Journal of Women's Health Physical Therapy. 2009;33(2):15-22.
- Thomas H. Obstetric Lecture: ATSU; 2012
Images:
http://coffeescholar.files.wordpress.com/2011/02/diastasis-recti-2.jpg
Lee D. Diastasis rectus abdominis and portpartum health. 2012; http://dianelee.ca/education/article_diastasis.php.
