Muscle imbalances
Transverse Abdominus (TrA) acts synergistically with pelvic floor activation and this feed-forward mechanism functions to create increased muscular activity in the TrA muscle just prior to the pelvic floor movement. Pelvic floor function relates to stability in the sacroiliac (SI) joint and pelvic ring. Pelvic floor muscle contraction stabilizes the SI joint lending to greater pelvic stability as demonstrated by the Active Straight Leg Raise test (ASLR). This deep, local muscle system plays a critical role in postural support and control, lumbopelvic control, generation of intra-abdominal pressure, and continence and respiration.
Key J. The pelvic crossed syndromes: a reflection of imbalanced function in the myofascial envelope; a further exploration of Janda's work. J Bodyw Mov Ther. 2010;14(3):299-301. Epub 2010 Mar 2014.
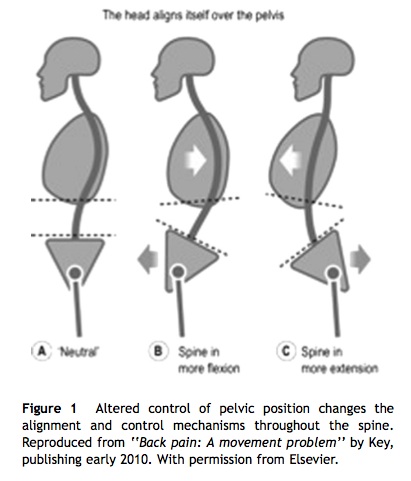
Pelvic crossed syndrome, as proposed by Janda, is imbalanced muscle activity leading to structural changes which may be the cause of pelvic pain. Tightness and over activity of the hip flexors and low back extensors with co-existing under activity of abdominals and gluteals create a "crossed" pattern of disturbed sagittal lumbopelvic postural movement and control.
signs and symptoms
- Pelvic pain
- Low back pain
- Pelvic asymmetry
- Postural asymmetry (sagittal / coronal plane)
- Excessive spinal curvature (lumbar lordosis/thoracic kyphosis)
physical therapy implications
- Postural control training and education
- Motor control training for local muscle system
- Core training
- Stretching of short and strong muscles
- Strengthening of long and weak muscles
adductor muscle lesion
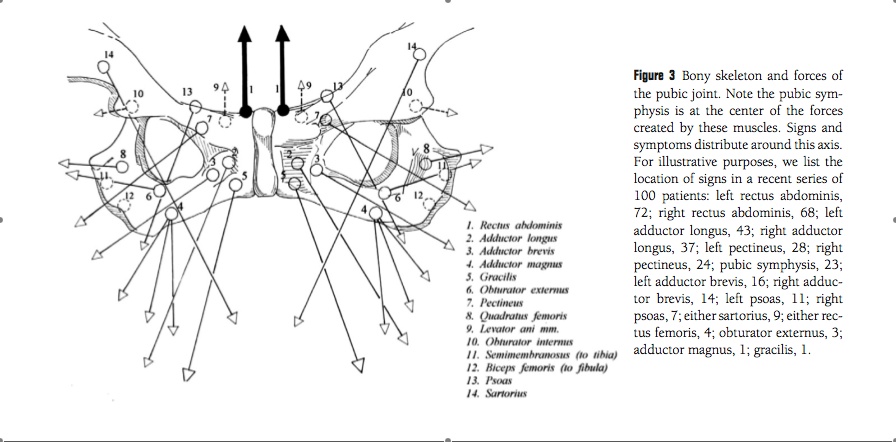
The adductor muscle group are vulnerable to shearing forces from unilateral loads and tremendous torque from the pelvis. Gracilis, pectineus and adductor longus are most often injured/avulsed during forceful hyperabduction of the hip with hyperextension of the abdominals in a movement such as kicking. This area is most vulnerable as demonstrated by Figure 3. There are 3 sets of forces and counterforces acting on the pubic symphysis:
1) Anterior compartment (abdominals)
2) Posterior compartment (hamstrings and adductor magnus)
3) Medial compartment (gracilis, adductor longus, brevis, and obturator externus)
Any imbalance in one compartment can lead to tremendous torque at the pubic symphysis and its' muscle insertions are vulnerable to this torque.
1) Anterior compartment (abdominals)
2) Posterior compartment (hamstrings and adductor magnus)
3) Medial compartment (gracilis, adductor longus, brevis, and obturator externus)
Any imbalance in one compartment can lead to tremendous torque at the pubic symphysis and its' muscle insertions are vulnerable to this torque.
Meyers WC, Yoo E, Devon ON, et al. Understanding "Sports Hernia" (Athletic Pubalgia): The Anatomic and Pathophysiologic Basis for Abdominal and Groin Pain in Athletes. Operative Techniques in Sports Medicine. 2007;14(4):165-177.
signs and symptoms
- Antalgic gait
- Pain with unipodal stance
- Pain with resisted adduction
- Pain and tenderness with palpation of adductor insertion
- Pain and tenderness with palpation of pubic symphysis
physical therapy implications
- Education on modification of painful activities
- Strengthening of abductors and hip external rotators
- Stretching of hip adductors (specific to short and tight adductors)
- Soft tissue mobilization to dysfunctional muscles
- Joint mobilizations to hip
references
Meyers WC, Yoo E, Devon ON, et al. Understanding "Sports Hernia" (Athletic Pubalgia): The Anatomic and Pathophysiologic Basis for Abdominal and Groin Pain in Athletes. Operative Techniques in Sports Medicine. 2007;14(4):165-177.
Key J. The pelvic crossed syndromes: a reflection of imbalanced function in the myofascial envelope; a further exploration of Janda's work. J Bodyw Mov Ther. 2010;14(3):299-301. Epub 2010 Mar 2014.
Apte G, Nelson P, Brismee JM, Dedrick G, Justiz R, 3rd, Sizer PS, Jr. Chronic female pelvic pain--part 1: clinical pathoanatomy and examination of the pelvic region. Pain Pract. 2012;12(2):88-110.
Key J. The pelvic crossed syndromes: a reflection of imbalanced function in the myofascial envelope; a further exploration of Janda's work. J Bodyw Mov Ther. 2010;14(3):299-301. Epub 2010 Mar 2014.
Apte G, Nelson P, Brismee JM, Dedrick G, Justiz R, 3rd, Sizer PS, Jr. Chronic female pelvic pain--part 1: clinical pathoanatomy and examination of the pelvic region. Pain Pract. 2012;12(2):88-110.
